Sebaceous Cyst
(Synonyms: sebaceous cysts Or trichilemmal cysts)
The vast majority of epidermoid or pilar cysts are of no great consequence but some in certain places are a cause for concern:
Epidermal cysts (also known as epithelial or infundibular cysts are intradermal or subcutaneous tumours. Epidermoid cysts may occur anywhere on the body but occur most often on the face, scalp, neck, back and scrotum.
Pilar cysts (also called trichilemmal cysts) are clinically indistinguishable from epidermal cysts. They contain keratinous material, are usually multiple and there is often an autosomal dominant inheritance.
Commonness of sebaceous cyst
Extremely common and probably most people will have one over the course of a lifetime. Often resolve spontaneously.
They are said to be twice as common in men as in women and most frequent in those aged in their 20s and 30s.
Simple epidermoid cysts can run in families.
Pilar cysts occur in 5-10% of the population. Over 90% occur on the scalp, where pilar cysts are the most common cutaneous cyst.
Appearance
Most often they present as a painless skin lump.
They may present with discharge of a foul cheese-like material. If they become infected, they are red, inflamed and painful.
Lesions of the genitals can be painful during intercourse and cause problems with walking or wearing underwear. They can also interfere with micturition.
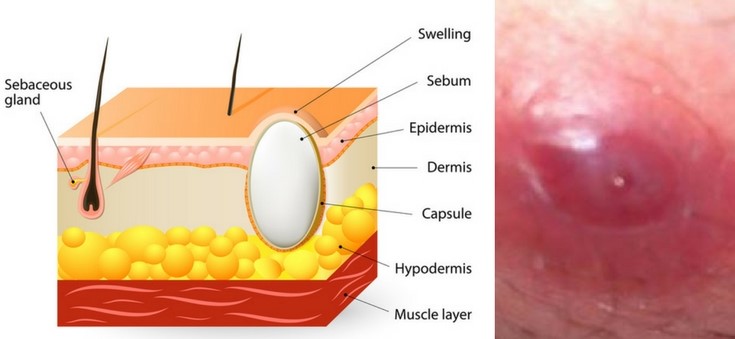
Epidermoid and pilar cysts appear as firm, round, mobile, flesh-coloured to yellow or white subcutaneous nodules of variable size.
A central pore or punctum may tether the cyst to the overlying epidermis and a thick cheesy material can sometimes be expressed. In people with dark skin, the cysts may also be pigmented.

Sites affected
The sites most commonly affected are, in descending order of frequency, the face, the trunk, the neck, the extremities, and the scalp.
Cysts of the genitals are less common and may appear as a mass in the vulva, the clitoris, the penis, the scrotum, or the perineum. In cultures that practice female circumcision (or female genital mutilation) cysts on the vulva are common.
The ocular and oral mucosa can also be affected, and cysts have been reported on the palpebral conjunctivae, on the lips, on the buccal mucosa, on and under the tongue, and even on the uvula. These are not sites with hair follicles.
Cysts may occur on the extremities. Subungual cysts can cause changes in the nails, such as onycholysis and subungual hyperkeratosis, which may be mistaken for psoriasis or onychomycosis. These cysts also produce changes in the nails (such as pincer nails) erythema, oedema, tenderness, and pain. Palmoplantar lesions represent a unique subset of epidermoid cysts.
Distinguished interpretation
Other causes of skin cysts.
A lipoma tends to be larger and is very soft. A neurofibroma is hard and may be multiple.
An abscess is hot and red and may resemble an infected sebaceous cyst. Multiple cysts in a teenager may suggest Gardner’s syndrome.
An intracranial epidermoid cyst (very rare) must be differentiated from a dermoid cyst, teratoma, schwannoma, glioma, craniopharyngioma and cavernous angioma.
Related conditions
Epidermoid cysts are a feature of Gardner’s syndrome. Gardner’s syndrome is an autosomal dominant condition comprising familial polyposis coli, cutaneous cysts and osteomas or other soft-tissue tumours. The cysts tend to occur at an earlier age than usual (presenting most often in the early teenage years). The face may be involved but the extremities tend to be affected more than the trunk.
Management
Most people with an epidermoid or pilar cyst never seek medical attention. If a cyst is uncomplicated then masterly inactivity should be advised. T Patients who present with cysts often prefer Sebaceous cyst Treatment/Sebaceous cyst surgery.
If the Sebaceous cyst Treatment/Sebaceous cyst surgery is red and hot it is probably infected. An antibiotic effective against staphylococci should be used, eg flucloxacillin. Infection may be mixed and, in lesions of the scalp and anogenital area, anaerobic flora are more likely.
If the cyst has ruptured, the contents can be expressed. However the cyst may well re-form.
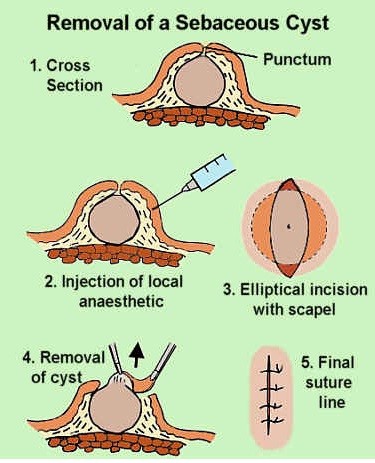
If the cyst is troublesome or if the patient, after counselling, Sebaceous cyst Treatment/Sebaceous cyst surgery, then it may be excised as a Sebaceous cyst Treatment/Sebaceous cyst surgery under the enhanced service of minor surgery. The entire cyst wall must be removed.
Excision of an epidermoid or pilar cyst
The usual preliminaries of informed consent are assumed. Information includes the warning that the cyst may recur if the entire wall is not removed.
Appropriate aseptic precautions should be taken.
Local anaesthetic such as 1% lidocaine with adrenaline is used (note contra-indications to use of adrenaline in certain areas). The area is infiltrated with local anaesthetic, being careful not to puncture the cyst.
The outlook (Prognosis)
They will usually grow slowly and only need removal if causing symptoms. They tend to recur if incised rather than excised.