Oesophageal cancer
Oesophageal cancer is cancer of the gullet (oesophagus). Most cases occur in people over the age of 55, although younger people are sometimes affected. Those diagnosed at an early stage have the best chance of a cure. The earliest symptom is often difficulty with swallowing (dysphagia). In general, the more advanced the cancer (the more it has grown and spread), the less chance that treatment will be curative. Most cases are diagnosed when the cancer is advanced. However, treatment can often slow the progress of the cancer or ease symptoms.
What is the oesophagus?
The oesophagus (gullet) is part of the gut (gastrointestinal tract). When we eat, food goes down the oesophagus into the stomach.
The upper section of oesophagus lies behind the windpipe (trachea). The lower section lies between the heart and the spine.
There are layers of muscle in the wall of the oesophagus.
These tighten (contract) to propel food down into the stomach.
There is a thickened circular band of muscle (a sphincter) at the junction between the oesophagus and stomach. This relaxes to allow food down, but normally tightens up and stops food and acid leaking back up (refluxing) into the oesophagus. In effect, the sphincter acts like a valve.
Knowing cancer
Cancer is a disease of the cells in the body. The body is made up from millions of tiny cells. There are many different types of cell in the body, and there are many different types of cancer
which arise from different types of cell. What all types of cancer have in common is that the cancer cells are abnormal and multiply out of control.
A malignant tumour is a lump or growth of tissue made up from cancer cells which continue to multiply. As they grow, malignant tumours invade into nearby tissues and organs, which can cause damage.
Malignant tumours may also spread to other parts of the body. This happens if some cells break off from the first (primary) tumour and are carried in the bloodstream or lymph channels to other parts of the body. These small groups of cells may then multiply to form secondary tumours (metastases) in one or more parts of the body. These secondary tumours may then grow, invade and damage nearby tissues, and spread again.
Some cancers are more serious than others, some are more easily treated than others (particularly if diagnosed at an early stage), some have a better outlook (prognosis) than others. So, cancer is not just one condition. In each case it is important to know exactly what type of cancer has developed, how large it has become, and whether it has spread. This will enable you to get reliable information on treatment options and outlook.
An insight into oesophageal cancer
Oesophageal cancer is cancer of the gullet (oesophagus). However, over a period of 20 years or so the number of cases diagnosed each year has risen. There are two main types:
Adenocarcinoma of the oesophagus. This occurs in about 6 out of 10 cases. This type arises from cells within mucous glands. (The lining of the oesophagus contains many tiny glands which make mucus. The mucus helps food to slide down into the stomach easily.) This type mainly occurs in the lower third of the oesophagus.
Squamous cell carcinoma of the oesophagus. This occurs in about 4 out of 10 cases. This type arises from cells which are on the inside lining of the oesophagus. This type mainly occurs in the upper two thirds of the oesophagus.
The symptoms, treatment and outlook are similar for both of these types. (There are some rare types of cancer which arise from other cells in the oesophagus.)
What causes oesophageal cancer?
A cancerous tumour starts from one abnormal cell. The exact reason why a cell becomes cancerous is unclear. It is thought that something damages or alters certain genes in the cell. This makes the cell abnormal and multiply out of control.
Many people develop cancer of the gullet (oesophagus) for no apparent reason. However, certain risk factors increase the chance that oesophageal cancer may develop. These include:
Ageing. It is more common in older people. Most cases are in people over the age of 55. It is also more common in men.
Diet is probably a factor. A high-fat diet is thought to increase the risk and eating a lot of fruit and green vegetables is thought to reduce the risk. Obesity may increase the risk too.
Where you live. Oesophageal cancer is much more common in China and certain other Far Eastern countries than in Europe. This may be due to dietary factors, or some other environmental factor.
Smoking.
Drinking a lot of alcohol, especially spirits.
Long-standing acid reflux from the stomach (gastro-oesophageal reflux disease (GORD)). This condition is common and causes inflammation at the lower end of the oesophagus. However, it has to be stressed that the risk is small – most people with acid reflux do not develop cancer.
Barrett’s oesophagus. This is a condition at the lower end of the oesophagus where the cells which line the oesophagus have become changed. In many cases this is related to long-term inflammation caused by acid reflux. The changed cells have an increased risk of becoming cancerous. About 1 in 100 people with Barrett’s oesophagus develop adenocarcinoma of the oesophagus at some stage.
Other uncommon conditions are associated with an increased risk and include:
Achalasia – a condition which causes a widening at the bottom of the oesophagus.
Tylosis – a very rare inherited skin condition.
Paterson-Brown-Kelly syndrome – a rare syndrome which includes iron deficiency and changes in the mouth or oesophagus.
Long-term exposure to certain chemicals and pollutants (chemical carcinogens) may irritate the oesophagus if you breathe them in and may increase the risk.
One recent study found that drinking black tea at temperatures of 70°C or higher increases the risk. Another study has found that people who get a flushed face when they drink alcohol also have a greater risk of developing oesophageal cancer when they also drink alcohol. This is because they lack an enzyme called aldehyde dehydrogenase.
Oesophageal cancer is not inherited so does not run in families. However, a family history of hiatal hernia appears to be a risk factor in developing oesophageal adenocarcinoma.
Expression of oesophageal cancer
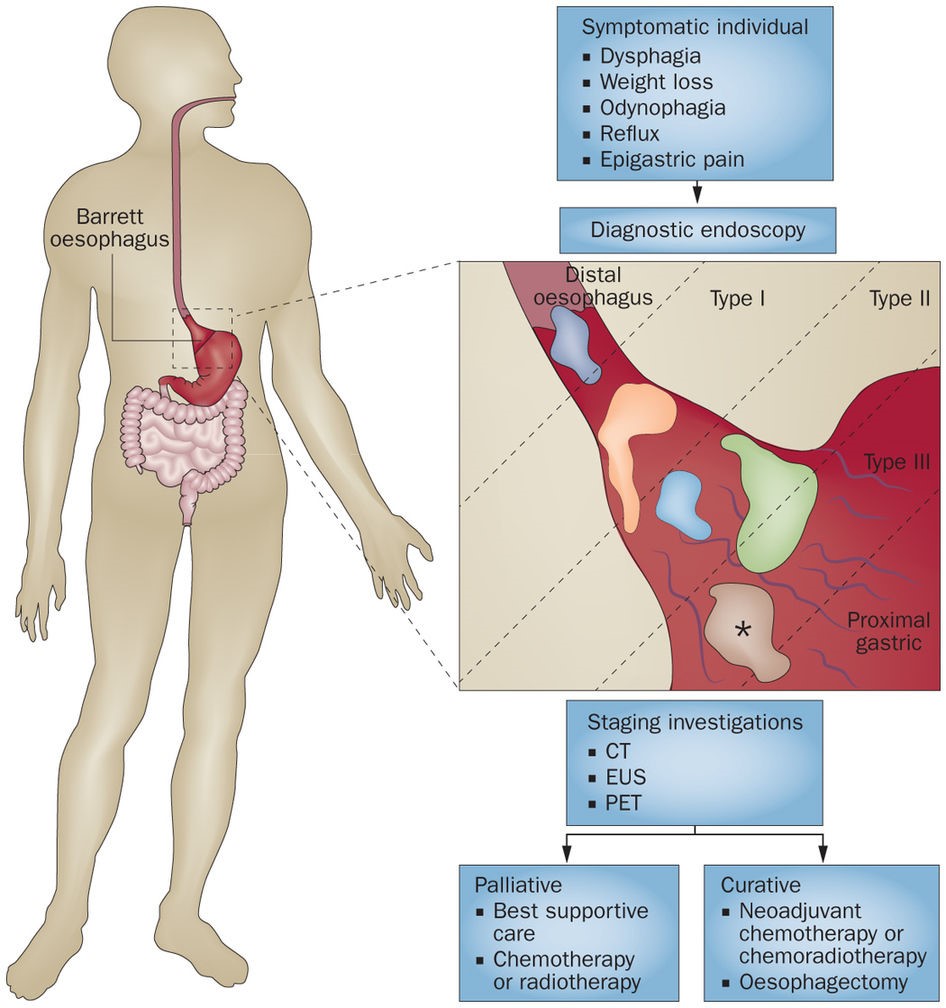
When a cancer of the gullet (oesophagus) first develops and is small it usually causes no symptoms. Some do not cause symptoms until they are quite advanced. As the cancer grows the symptoms which may develop usually include one or more of the following:
Difficulty with swallowing (dysphagia). This is often the first symptom and is caused by a tumour narrowing the passage in the oesophagus. Food may appear to stick as you try to swallow. If it gets worse then drinks may also be difficult to swallow.

Being sick (vomiting) after eating (which is really regurgitating food which has become stuck). Pain in the chest or in the back of the chest when you swallow (odynophagia).
Weight loss
Vomiting blood.
Coughing. Particularly when you swallow.
A hoarse voice.
Acid reflux symptoms may first develop, or get worse, when you develop a cancer at the lower oesophagus next to the stomach. Symptoms include pains in the chest (heartburn).
Note: acid reflux is common and most people with acid reflux do not have cancer.If the cancer spreads to other parts of the body, various other symptoms can develop.
All the above symptoms can be due to other conditions, so tests are needed to confirm oesophageal cancer.
Identification and assessment of oesophageal cancer
Initial assessment and gastroscopy (endoscopy)
If a doctor suspects that you may have cancer of the gullet (oesophagus), he or she will examine you to look for signs such as a lump in your tummy (abdomen). The examination is often normal, especially if the cancer is at an early stage. Therefore, a gastroscopy is usually arranged.
A gastroscope (endoscope) is a thin, flexible telescope. It is passed through the mouth, into the oesophagus and down towards the stomach. The endoscope contains fibre-optic channels which allow light to shine down so the doctor or nurse can see inside.
Biopsy – to confirm the diagnosis
When a small sample of tissue is removed from a part of the body, the procedure is called a biopsy. The sample is then examined under the microscope to look for abnormal cells. When you have a gastroscopy, if anything abnormal is seen, the doctor or nurse can take a biopsy. This is done by passing a thin grabbing instrument down a side channel of the gastroscope. It can take two weeks for the result of a biopsy.
Assessing the extent and spread
If you are confirmed to have oesophageal cancer, further tests may be done. For example, a special ultrasound scan, which uses a probe at the end of a gastroscope, can assess how far the cancer has grown through the wall of the oesophagus.
Other tests may be arranged to see if the cancer has spread to other parts of the body. For example, a CT scan, an ultrasound scan of the abdomen, or other tests.
This assessment is called staging of the cancer. The aim of staging is to find out:
How much the tumour in the oesophagus has grown, and whether it has grown partially or fully through the wall of the oesophagus.
Whether the cancer has spread to local lymph nodes.
Whether the cancer has spread to other areas of the body (metastasised).
By finding out the stage of the cancer it helps doctors to advise on the best treatment options. It also gives a reasonable indication of outlook (prognosis).
Doctoring oesophageal cancer
Treatment options which may be considered include surgery, chemotherapy and radiotherapy. The treatment advised for each case depends on various factors, such as:
The exact site of the primary tumour in the gullet (oesophagus).
How large the cancer is and whether it has spread (the stage of the cancer).
Your general health.
You should have a full discussion with a specialist who knows your case. They will be able to give the pros and cons and the likely success rate for your type of cancer. They will also be able to outline possible side-effects and other details about the possible treatment options.
You should also discuss with your specialist the aims of treatment. For example:
Treatment may aim to cure the cancer. Some cancers of the oesophagus can be cured, particularly if they are treated in the early stages of the disease. (Doctors tend to use the word remission rather than the word cured. Remission means there is no evidence of cancer following treatment. If you are in remission, you may be cured. However, in some cases a cancer returns months or years later. This is why doctors are sometimes reluctant to use the word cured.)
Treatment may aim to control the cancer. If a cure is not realistic, with treatment it is often possible to limit the growth or spread of the cancer so that it progresses less rapidly. This may keep you free of symptoms for some time.
Treatment may aim to ease symptoms. If a cure is not possible, treatments may be used to reduce the size of a cancer, which may ease symptoms such as pain or difficulty with swallowing. If a cancer is advanced, you may require treatments such as nutritional supplements, painkillers, or other techniques to help keep you free of pain or other symptoms.
Surgery
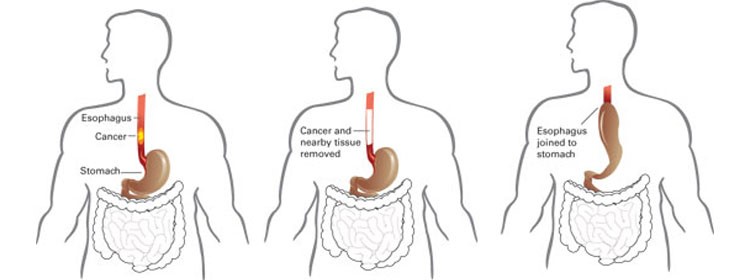
It may be possible to remove the tumour. To do this, the operation is to remove part or all of the oesophagus, depending on the site and size of the tumour.
There are various ways a surgeon can get to the oesophagus and various types of operation. If the lower part of the oesophagus is removed, it may be possible to sew the stomach back on to the remaining section of oesophagus if the stomach is brought up into the chest area. If all of the oesophagus is removed, the surgeon may use a section of your gut (intestine) to create a new artificial oesophagus. Some lymph glands around the oesophagus are also removed at the same time of the operation to see if any cancer has spread to them.
Radiotherapy
Radiotherapy is a treatment which uses high-energy beams of radiation which are focused on cancerous tissue. This kills cancer cells, or stops cancer cells from multiplying.
When radiotherapy is used to treat cancer of the oesophagus it is commonly used in addition to either surgery or chemotherapy. The exact combination of treatments advised depends on various factors.
Two types of radiotherapy are used for oesophageal cancer – external and internal:
External radiotherapy. In this procedure, radiation is targeted on the cancer from a machine. (This is the common type of radiotherapy which is used for many types of cancer.)
Internal radiotherapy (brachytherapy). This treatment involves placing a small radioactive implant next to the cancerous tumour for a short time. It is then removed. (It is put in position via the oesophagus, usually by a gastroscope (endoscope).
A newer treatment called photodynamic therapy (PDT) uses low-powered lasers combined with a light-sensitive medicine to destroy cancer cells. It is more commonly used as a treatment to relieve the difficulty in swallowing caused by cancer of the oesophagus. PDT is being used in trials for the treatment of early oesophageal cancer, instead of surgery.
The outlook (prognosis) for oesophageal cancer
Without treatment, cancer of the gullet (oesophagus) is likely to get larger, and spread to other parts of the body. If it is diagnosed and treated at an early stage, there is a chance of a cure with treatment. An ‘early stage’ would be before the cancer has grown through the wall of the oesophagus or spread to lymph nodes or other areas of the body. Unfortunately, most cases are not diagnosed at an early stage. This is because symptoms do not tend to develop until the cancer is already fairly large.
If the cancer is diagnosed when it has grown through the wall of the oesophagus, or spread to other parts of the body, a cure is less likely. However, treatment can often slow down the progression of the cancer. Currently, about a quarter of people diagnosed with oesophageal cancer are still alive five years after diagnosis.
Studies have suggested that a combination of the treatment esomeprazole – a type of medicine known as a proton pump inhibitor – and low-dose aspirin may help in preventing the development of oesophageal adenocarcinoma. Further evaluation of this finding is now ongoing.
The treatment of cancer is a developing area of medicine. New treatments continue to be developed and the information on outlook above is very general. The specialist who knows your case can give more accurate information about your particular outlook, and how well your type and stage of cancer is likely to respond to treatment.
Even if the cancer is advanced and it is not possible to remove it, some surgical techniques may still have a place to ease symptoms. For example, a blockage may be eased by:
Using laser surgery.
Inserting a rigid tube (a stent).
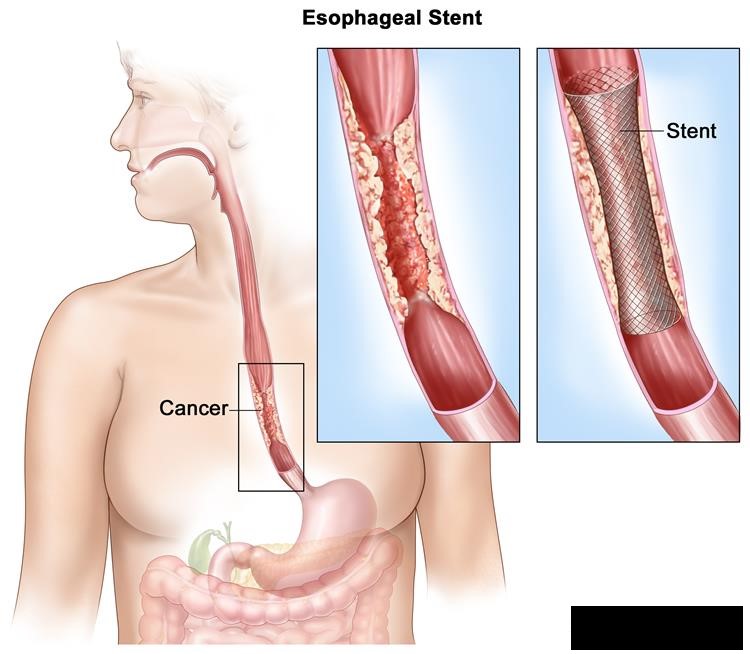
Stretching of the oesophagus, which allows food and drink to pass through the blockage to the stomach.
Chemotherapy
Chemotherapy is a treatment of cancer by using anti-cancer medicines which kill cancer cells, or stop them from multiplying.
Chemotherapy may be used in addition to surgery or radiotherapy. For example, following surgery you may be given a course of chemotherapy. This aims to kill any cancer cells which may have spread away from the primary tumour. When chemotherapy is used after surgery it is called adjuvant chemotherapy. In some cases, chemotherapy is given before surgery, to shrink a large tumour so that surgery is more likely to be.