Pilonidal Sinus
Pilonidal Sinus & Abscess
Pilonidal is a condition in which hair grows/collected under the skin in natal cleft (Space between two buttocks). Pilonidal sinus is an abnormal track from deeper infection below to the skin.
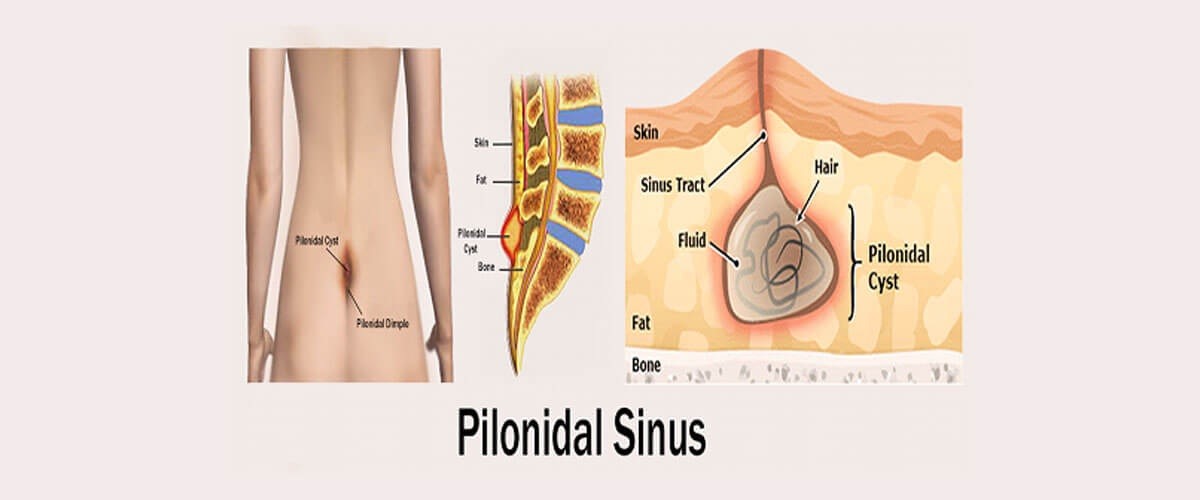
The track usually travels vertically which may progress with time.
The exact cause of the pilonidal sinus is not known. Some people are born with a pit where hair is trapped between buttocks and with age. sinus develops. In some cases the pit may develop with constant pressure. Some of the conditions which increases the incidence includes
1. A job involving a lot of sitting (a sedentary occupation)
2. Being overweight (obesity)
3. A previous persistent irritation or injury to the affected area
4. Having a hairy, deep natal cleft
5. A family history of the condition
6. Drivers

Treatment Options:
Laser Pilonidal Sinus Treatment/Laser Pilonidal Sinus surgery
Laser Pilonidal Sinus Treatment/Laser Pilonidal Sinus surgery has now revolutionised treatment of pilonidal sinus. All the treatment options discussed above involve big scar, pain and intensive wound management. In addition Laser Pilonidal Sinus Treatment/Laser Pilonidal Sinus surgery they alter ones work/life balance significantly for about 6 -8 weeks.
Laser Pilonidal Sinus Treatment/Laser Pilonidal Sinus surgery Surgery overcomes all the disadvantages of the traditional surgery. Advantages are
1. Scar is minimal seen only at pits
2. Pain is minimal compared to other procedures
3. Wound management is minimal
4. One can return to work quicker
Laser Pilonidal Sinus Treatment/Laser Pilonidal Sinus surgery is usually combined with Endoscopic Pilonidal Sinus Treatment (EPSiT) leading to higher success rate.
These advantages make Laser Pilonidal Sinus Treatment/Laser Pilonidal Sinus surgery widely acceptable.
Traditional Treatment for Pilonidal Sinus
1. When the abscess develops in a short span of time (Acute abscess) and pain and infection are not severe then it can be treated with course of antibiotics for 5 days and planned definitive surgery with in 6 weeks.
2. When the abscess develops in a short span of time (Acute abscess) and pain and infection are severe then it can be treated with immediate excision
3. When it's a recurrent chronic condition then planned surgery is done.
I offer the following surgical options depending on the condition
1. If infection is less and there is no contamination of surgical site then excision and primary closure.
2. If surgical site is contaminated then excision and healing by secondary intention.
Both above procedures are simple with no other added complications and will be enough to treat about 95% conditions so I would always prefer to perform simple wide excision +/- primary closure for all the pilonidal conditions as a first choice. If condition recurs then an advanced procedure which involves mobilising and closure with flap can be performed. Pilonidal sinus is minor condition but problematic because of the place it affects.