Achalasia
The oesophagus and the sphincter
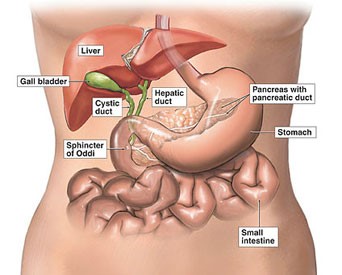
The gullet (oesophagus) contains muscles. These muscles contract in a rhythmic way to allow food to pass down the oesophagus. This is known as peristalsis. At the lower end of the oesophagus there is a ring of muscle called a sphincter. This sphincter relaxes to allow food to pass from the oesophagus into the stomach. But, when no food is passing down the sphincter contracts to stop food passing back up (refluxing) into the oesophagus
Understanding Achalasia
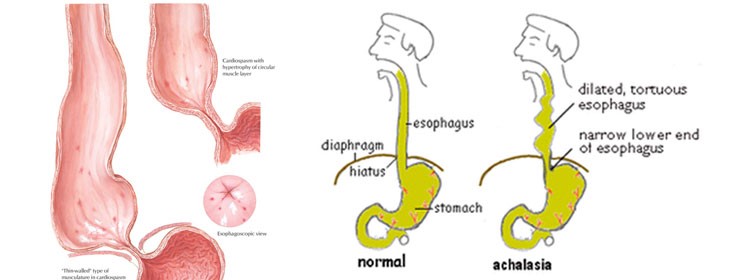
Both muscles and nerves are present in the gullet or oesophagus. Both the muscles and the nerves of the oesophagus are affected by achalasia, especially initially the nerves that cause the sphincter between the oesophagus and stomach to relax. The muscles do not contract properly so the rhythmic contraction of muscles, which allows food to pass down the oesophagus (peristalsis), does not occur correctly. In addition, the sphincter does not relax properly so food cannot pass through into the stomach easily. This makes it difficult for one to swallow food properly. This leads to the main part of your oesophagus then becoming enlarged and widened (dilated) with time.
Prevalence and effects of Achalasia
About 1 in 100,000 people are diagnosed with achalasia each year which evidently makes it an uncommon condition.. Mainly adults aged between 20-40 years are affected by it. In most cases, no underlying cause can be found and the reason why the nerves and muscles in the gullet (oesophagus) do not work so well is not clear.
Indications of Achalasia
1. Difficulty in swallowing (dysphagia) both food and liquids is the most common symptom.
2. One may also feel that some of the food eaten is as if getting stuck in the chest after one has eaten.
3. One may also commonly lose weight, as one cannot swallow all the food.
4. In some cases some chest pains or a heavy sensation on the chest may be felt.
5. Some people also develop a cough, which is sometimes worse at night.
6. Heartburn is also fairly common.
7. As one’s gullet (oesophagus) dilates, one may find that some of the food is brought back up (regurgitated). If this happens during the night one may experience some choking or coughing.
Investigations for Achalasia
Most people will have had achalasia for a length of time, even for years, before the diagnosis is made. Various investigations may be advised if one’s doctor feels the probability of achalasia. These usually include one or more of the following:
Barium swallow
This is a specialised X-ray test. In this test, X-rays of the gullet (oesophagus) are taken after one swallows a liquid called barium, which shows up as white on the X-ray. This test will show if the oesophagus is dilated. It will also show if the barium stays in one’s oesophagus for longer than normal.
Manometry
In this test, the pressure that is generated within one’s oesophagus when one swallows is monitored. During this test, a thin tube is inserted through one’s nose, down the back of one’s throat and into the oesophagus. This test can often detect earlier changes than a barium swallow can.
Gastroscopy – sometimes called endoscopy
Under gastroscopy, gastroscope (endoscope) which is a thin, flexible telescope is passed through the mouth, into the oesophagus and down towards the stomach and the first section of the intestine (the duodenum). The endoscope contains fibre-optic channels which allow light to shine down so the doctor or nurse can see inside one’s oesophagus, stomach and duodenum.
Curing achalasia
There are different treatments available. These include:
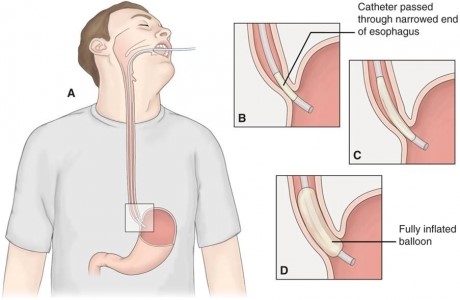
1. Dilatation
A procedure in which the sphincter is made wider (dilated) is called dilatation. This is done by using a balloon which is inflated to stretch the sphincter. This is done with the use of a gastroscope, to ensure the balloon is in the correct position.
2. Medication
Help of various medicines can be taken to relax the sphincter at the lower end of the gullet (oesophagus). Examples include Nitrates & Calcim channnel blockers.These work best when achalasia is first diagnosed. However, they usually only work in the short term and are most often prescribed for people who cannot have other forms of treatment.
3. Botulinum toxin
Botulinum toxin is another method of treating achalasia where it acts as a muscle relaxant and is injected into the sphincter to weaken the muscle. This is usually a safe treatment. However, it only works for a few months, so further injections are often necessary. It may be more suitable for people who are unable to have surgery.
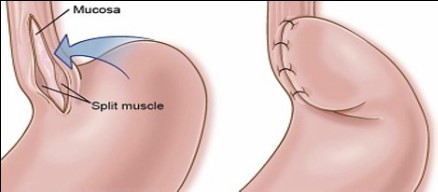
4. Operation
In some cases a keyhole surgery may be performed. Under this muscle fibres in the sphincter are divided (cut) during an operation. This is often done by keyhole surgery. This is usually very successful at easing the symptom of difficulty swallowing.
However, it may cause complications such as gastro-oesophageal reflux disease. This is a condition where the acid from one’s stomach comes up into one’s oesophagus and can cause heartburn.
CONCLUSION
An uncommon condition that affects the muscles of the gullet (oesophagus), is termed as Achalasia.. It usually causes difficulty in swallowing both food and fluids. There are different ways of dealing with achalasia to improve symptoms