Carcinoid Tumour
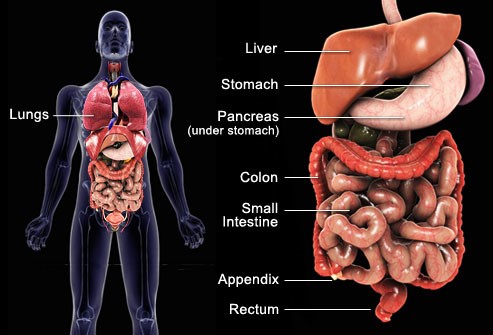
Carcinoid tumours are neuroendocrine tumours (NETs) of predominantly enterochromaffin cell origin (Kulchitsky cells). Two thirds of carcinoid tumours occur somewhere in the gastrointestinal tract. The small intestine is the most frequent location, followed by the lungs or bronchi, rectum, appendix and stomach. Carcinoid tumours account for about two-thirds of neuroendocrine gastroenteropancreatic tumours. 30% of intestinal NETs are associated with carcinoid syndrome.
Carcinoid tumours are often indolent asymptomatic tumours. However, a small but significant proportion is malignant and difficult to manage. Metastases to the mesenteric lymph nodes, liver, ovaries, peritoneum and spleen may occur. Carcinoid tumours may secrete various bioactive compounds, including serotonin and bradykinin, which cause carcinoid syndrome, which includes bronchospasm, diarrhoea, skin flushing, and right-sided valvular heart lesionsCarcinoid tumours of the ileum and jejunum, especially those larger than 1 cm, are most likely to cause carcinoid syndrome.
Neuroendocrine tumours of the lung account for 1%-2% of all lung cancer. About 70% of all carcinoids are located in the major bronchi and the remainder in the periphery of the lungs. They occur more frequently in the right than in the left lung, and especially in the middle lobe.
Epidemiology
Carcinoid tumours are the most common neuroendocrine tumours.
The incidence of neuroendocrine tumours diagnosed during life is increasing, with the majority being gastrointestinal carcinoid tumours. Recent studies have estimated an annual incidence of approximately 3 per 100,000 per year.
Carcinoid tumours may be found as an incidental finding in up to 10% of postmortem examinations. The risk is increased if there is a family history involving a first-degree relative
Presentation
Most tumours are clinically silent, but they may cause pain, weight loss or present as a palpable mass.
Carcinoid tumours may produce vague right-sided abdominal discomfort but any symptoms are usually mild and have often been present for a number of years before a diagnosis is made. Diagnosis may be made after urgent surgery, eg for gastrointestinal obstruction.
Carcinoid heart disease:
Endocardial fibrosis may occur, especially in patients with hepatic metastases.
The right side of the heart is most often affected, especially tricuspid valve regurgitation; however, tricuspid stenosis, pulmonary regurgitation and pulmonary stenosis may occur. , Left heart lesions may occur in patients with pulmonary metastases.
Carcinoid tumours may also cause fibrosis, including retroperitoneal fibrosis, and so presentation may include features such as hydronephrosis (obstruction of the ureter), mesenteric ischaemia or Peyronie’s disease.
In patients with widely metastatic carcinoid tumours, increased conversion of tryptophan to serotonin may lead to tryptophan and niacin deficiency, presenting as hypo albuminaemia and pellagra.
Examination is often normal but may reveal a right-sided abdominal mass, hepatomegaly, telangiectasia, pellagra, and tricuspid regurgitation.
Carcinoid syndrome
Classic carcinoid syndrome occurs in fewer than 10% of patients with carcinoid tumours, and occurs most often in patients with carcinoid tumours in the small intestine, appendix and proximal large bowel.
Features of carcinoid tumours are caused by the release of pharmacologically active mediators 5-hydroxytryptamine (5-HT), prostaglandins, kinins, substance P, gastrin, somatostatin, corticotrophin and neuron-specific enolase into the peripheral circulation.
Secretion of bioactive substances varies depending on the location of the tumour and the presence of metastases.
Presentation:
Flushing (especially after alcohol, coffee, various foods or drugs).
Other features include diarrhoea, abdominal pain, palpitations, hypotension and wheezing.
Carcinoid syndrome variants may be seen in patients with bronchial and gastric carcinoid tumours; for example:
Gastric carcinoid tumours may cause flushing which is pruritic and well-demarcated, and an increased incidence of peptic ulcer.
Bronchial carcinoid tumours may cause flushing which lasts for days and is often associated with changes in mental state.
Differential diagnosis
Other possible causes of site-related tumours.
Other causes of flushing (carcinoid syndrome), eg alcohol, nitrates, spicy foods, systemic mastocytosis, medullary thyroid cancer, menopause, renal cell cancer, hyperthyroidism.
Other causes of diarrhoea, eg gastroenteritis inflammatory bowel disease.
Other causes of bronchospasm, eg anaphylaxis, asthma, inhaled foreign body, chronic obstructive pulmonary disease.
Investigations
Plasma chromogranin A is an effective screening test because it is very sensitive but is not very specific.
24-hour urinary excretion of 5-hydroxyindoleacetic acid (5-HIAA): 24-hour excretion greater than 25 mg provides strong evidence for the diagnosis of carcinoid syndrome.
False positive results may occur with certain foods (eg bananas, kiwi fruit, pineapple, plums, tomato products) and some drugs (eg paracetamol, antipsychotics, some cough remedies, caffeine, diazepam, nicotine, warfarin).
False negatives may occur with various drugs, eg alcohol, aspirin, antidepressants.
Other baseline investigations, considering possible associated neuroendocrine neoplasia or bowel adenocarcinoma, include FBS, LFTs, TFTs, , parathyroid hormone, calcium, calcitonin, prolactin. alpha-fetoprotein, carcinoembryonic antigen (CEA) and beta-hCG.
Provocative tests (eg pentagastrin test) may be considered if other screening test results are equivocal; however, close monitoring and ready access to intravenous somatostatin are essential in case of a carcinoid crisis.
Gastric and intestinal tumours may be diagnosed by endoscopy or endoscopic ultrasound; barium studies may demonstrate polyps.
CT or MRI scanning and laparotomy may be needed for localisation.
Scintigraphic imaging with labelled somatostatin can provide accurate information on the site and dissemination of the tumour.
Somatostatin single-photon emission computer tomography (SPECT) may also be used.
In a young person whose pneumonia is slow to resolve, a bronchoscopy may reveal a carcinoid tumour.
Associated diseases
Carcinoid tumours are associated with multiple endocrine neoplasia (MEN) (MEN) type 1 in about 10% of cases. MEN 1 is the association of parathyroid adenoma, pancreatic islet cell tumour and pituitary adenoma.
Adenocarcinoma in 10-20% (usually colorectal adenocarcinoma).
Management
If metastases are present, avoid precipitating factors, eg alcohol, chocolate, spicy foods, strenuous exercise.
Treatment is usually based on the size of the tumour. Surgical resection (local resection with node clearance) when possible is the treatment of choice. Surgery should be considered for patients with liver metastases and potentially resectable disease.
Options for non-resectable disease include somatostatin analogues, eg octreotide (which blocks 5-HT release), biotherapy, targeted radionuclide therapy, radiofrequency ablation therapy and chemotherapy.
For advanced metastatic disease, somatostatin analogue therapy and surgical debulking provide the best symptomatic relief and may improve survival.
Chemotherapy drugs currently being assessed in trials to palliate metastatic carcinoid disease include alkylating agents, doxorubicin and 5-fluorouracil.
Interferon alfa is a useful additive therapy when symptoms of carcinoid syndrome do not resolve with a somatostatin analogue alone.
External beam radiotherapy may relieve bone pain from metastases.
Chemoembolisation of the hepatic artery may provide effective, short-term relief of symptoms due to hepatic metastasis.
Liver transplantation can be considered in selected cases, eg young patients without documentedspread outside the liver and resected primary tumour.
Complexities
Gastrointestinal carcinoid tumours may cause appendicitis, intussusceptions, bowel obstruction or bowel perforation (rare).
The tendency for metastatic spread increases with tumour size, and is substantially higher in lesions larger than 2.0 cm.
Carcinoid crisis:
Carcinoid crisis may dramatically worsen symptoms and be life-threatening.
The tumour may outgrow its blood supply and release large amounts of vasoactive mediators, causing cardiovascular collapse, tachycardia and altered mental state.
Carcinoid crisis may also occur during surgical removal but this can be prevented by octreotide infusion before surgical manipulation.
Management of carcinoid crisis includes infusion of octreotide and plasma.
The Outlook
Advances in diagnostic methods and surgical techniques have allowed more active management and improved prognosis.
The prognosis for patients with completely resected localised disease is excellent, but patients with metastases have poor outcome.
Prognosis depends on site. One large report from the USA found 5-year survival rates for stomach (75%), small intestine (76%), appendix (76%) and rectum (87%).
Median survival is 5-8 years but, if metastases are present, the mean is 38 months (8% survival at 4 years).
5-year survival for carcinoid tumours of the lung has been reported as 96% in one study (14% had lymph node involvement and none had carcinoid syndrome).