Cholangiocancer (Bileduct Cancer)
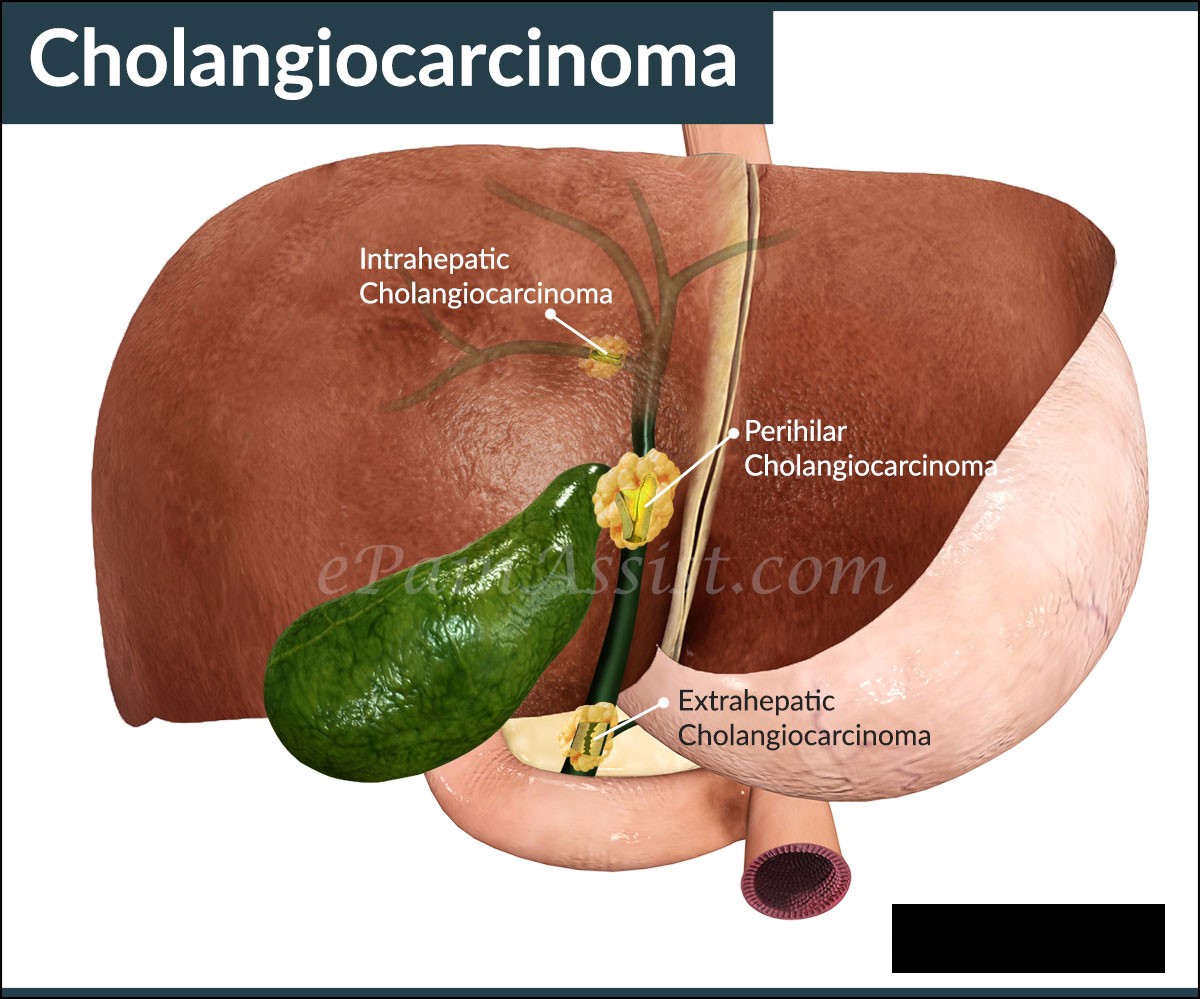
Cholangiocarcinoma is a carcinoma arising in any part of the biliary tree from the small intrahepatic bile ducts to the ampulla of Vater at the distal end of the common bile duct. More than 90% of cholangiocarcinomas are ductal adenocarcinomas and the remainder are squamous cell tumours.
Most commonly, they occur in the perihilar region (classical Klatskin’s tumour) near the bifurcation of right and left hepatic ducts.
Tumours occurring between the upper border of the pancreas and ampulla of Vater are the next most common and are classified as distal extrahepatic tumours.
Can also occur (least commonly) as an intrahepatic tumour.
Prevalence
Incidence is 1-2 per 100,000 population per year . Most cases occur in those aged over 60 years.
There is a high incidence of cholangiocarcinoma in Southeast Asian countries, due to chronic endemic parasitic infection with liver flukes.
In Japan and Israel the incidence is much higher at 5.5 and 7.3 cases per 100,000 people per year. The incidence of intrahepatic cholangiocarcinoma is increasing and the incidence is estimated as 0.9-1.3/100,00 for males and 0.4-0.7/100,000 for females. Intrahepatic cholangiocarcinoma accounts for 10-15% of primary liver cancer.
Risk factors
Patients with chronic ulcerative colitis who develop primary sclerosing cholangitis are prone to cholangiocarcinoma. The lifetime risk of developing this cancer is 10-20% with primary sclerosing cholangitis. Some patients with Crohn’s disease may also be at risk.
Infection with the liver flukes Clonorchis sinesis and Opisthorchis viverrini have been causally linked. Ascaris lumbricoides infectionhas also been implicated.
Industrial chemical exposure: chemicals used in the aircraft, rubber and wood-finishing industries have been implicated.
Thorium exposure is associated with an increase in cases of cholangiocarcinoma. Congenital abnormalities of the bile ducts, eg choledochal cysts.
Caroli’s disease (a rare congenital disorder of the intrahepatic bile ducts associated with autosomal recessive polycystic kidney where the bile ducts become chronically dilated.
Recently implicated potential risk factors for the intrahepatic form include hepatitis C, HIV, cirrhosis and diabetes.
Presentation
Jaundice is an early feature in perihilar tumours, usually .with hepatomegaly, Abdominal pain localised to the right upper quadrant, especially in advanced disease.
Weight loss is variable.
Pale-coloured stools, passage of dark urine, upper gastrointestinal pain (dull ache in the upper right quadrant), weight loss, anorexia and general malaise are common features.
Puritis maybe the presenting symptom predating jaundice on occasions.Hepatomegaly, Splenomegaly ispresent if prolonged biliary obstruction has caused secondarybiliary cirrhosis.
The presence of a palpable gallbladder (Courvoisier’s sign) may occur with tumours distal to the cystic duct
Investigations
Diagnosis should be made on the basis of radiological investigations (including CT or MRI) and pathological assessment from a biopsy, fine needle aspiration or biliary brush cytology.
LFTs: elevated conjugated bilirubin. Cholestatic picture with markedly elevated alkaline phosphatase,gamma-GT elevated with aminotransferases affected minimally.
Cogulation: Prothrombin time and INR may be prolonged.
Tumour markers: carbohydrate antigen (CA) 19-9 andCarcinoembryonic antigen (CEA)tumourmarkers may be raised (also found in other causes of obstructive jaundice.
Alpha-fetoprotein is not produced by cholangiocarcinoma.
Ultrasound and CT scan: hilar tumours show dilatation of intrahepatic biliary tree.
Contrast MRI is the optimal imaging for diagnosis of cholangiocarcinoma. However it is inferior to CT for detecting distant metastases.
MRI cholangiography or endoscopic retrograde cholangiopancreatography (ERCP) show the site of obstruction. ERCP may be used to obtain samples for biopsy or cytological analysis.
Angiography may be conducted as a prelude to surgical intervention, as encasement of the hepatic arteries or portal vein precludes successful surgical therapy.
Differential diagnosis
Acute cholecystitis
Bile duct strictures.
Extrabiliary tumour compressing biliary system.
Biliary adenoma.
Primary bilary cirrhosis
.Primary sclerosing cholangitis
Ascending cholangitis.
Obstructive choledocholithiasis
Pancreatic tumours
Choledochal cysts
Acute hepatitis.
Staging
Staging is based on the tumour, node and metastasis (TNM) classification with some modifications for intrahepatic cholangiocarcinoma, perihilar cholangiocarcinoma and distal cholangiocarcinoma. Hilar cholangiocarcinoma (Klatskin’s tumour) is clinically staged depending on the involvement of the hepatic ducts according to the Bismuth-Corlette classification Staging consists of:
Complete history and physical examination. Blood counts, LFTs.
CXR:Imaging of the abdomen by sonography and CT scan or MRI. Endoscopic retrograde or percutaneous transhepatic cholangiography.
Endoscopic ultrasonography, cholangioscopy and laparoscopy may be required.
Upper and lower gastrointestinal tract endoscopy has to be performed in patients with an isolated intrahepatic mass.
Management
Surgery
Complete surgical resection is the only intervention to offer a chance of cure but fewer than 33% are resectable at diagnosis.
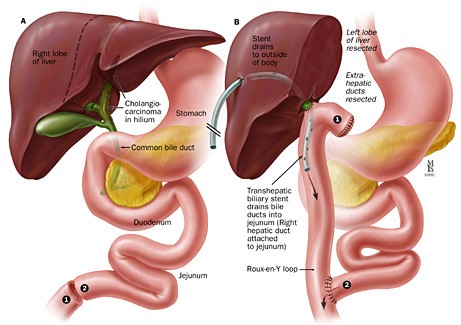
Intrahepatic and Klatskin tumours require liver resection.
Aggressive surgical resection (including liver resection ± liver transplantation with adjuvant Chemotherapy may offer a cure rate of around 30% in suitable candidates at the best centres. Palliative surgery is required if stenting cannot be achieved.
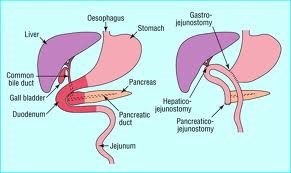
Surgical bypass procedures may be required for biliary obstruction, especially for tumours in the common bile duct.
Adjuvant chemotherapy is thought to be of benefit but there is no consensus on its effect or optimal regimens.
Adjuvant and preoperative radiation therapy has been used to reduce tumours in an effort to make them resectable. Radiotherapy without surgery, with or without chemotherapy, has been shown to improve survival in patients with inoperable or unresectable tumours.
Nonsurgical therapy
Postoperative treatment after non-curative resection of cholangiocarcinoma remains controversial, and both supportive care and palliative chemotherapy and/or radiotherapy may be considered.
Stents:
Endoscopic retrograde cholangiopancreatography (ERCP) may be used to stent the bile duct to relieve symptoms; they are prone to occlusion and may need replacing approximately every three months.
Self-expanding metal stents seem to offer the best technical outcome.
However, there is no evidence to support the benefit of ERCP with stenting in patients with malignant pancreaticobiliary diseases while awaiting surgery.
Primary radiotherapy, with or without chemotherapy, has shown a survival advantage and significant palliation over stent placement or bypass surgery alone in patients with medially inoperable or unresectable tumours.
Chemotherapy used without radiotherapy has not shown any significant local control or survival benefit.
Photodynamic therapy is an experimental treatment which may have some benefit, in terms of prolonging survival but is not currently recommended as part of routine management.
The reality for most patients is that their long-term survival is unlikely and good palliative symptom-relieving care is the mainstay of management.
Challenges
The risk of biliary tract sepsis is increased and may cause a deterioration which is amenable to antibiotic therapy.
Secondary biliary cirrhosis occurs in 10-20% of patients.
Prognosis
Progressive deterioration with average survival of 12-18 months from diagnosis. The overall survival rates are low because many patients present with unresectable or metastatic disease.
Even in patients undergoing aggressive surgery, five-year survival rates are 10-40% for cholangiocarcinoma.
Prognosis is much better for those with extrahepatic tumours who are suitable for early surgical intervention.
Intrahepatic lesions carry the worst prognosis.